
Choose Amyvid to aid in the clinical diagnosis of Alzheimer’s disease (AD) and the selection of patients who are indicated for amyloid beta–directed therapy1
Amyvid provides objective evidence
Amyvid PET scans estimate amyloid beta plaque density in adults with cognitive impairment to aid in the evaluation of Alzheimer’s disease (AD) and the selection of patients who may be eligible for amyloid beta–directed therapy.1
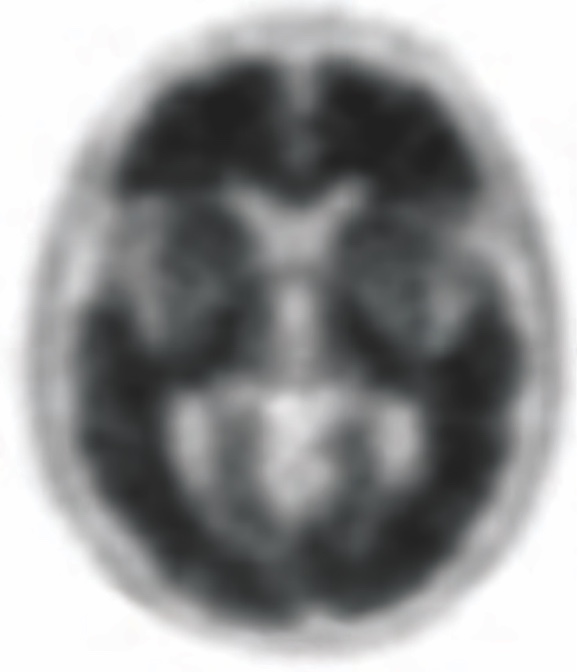
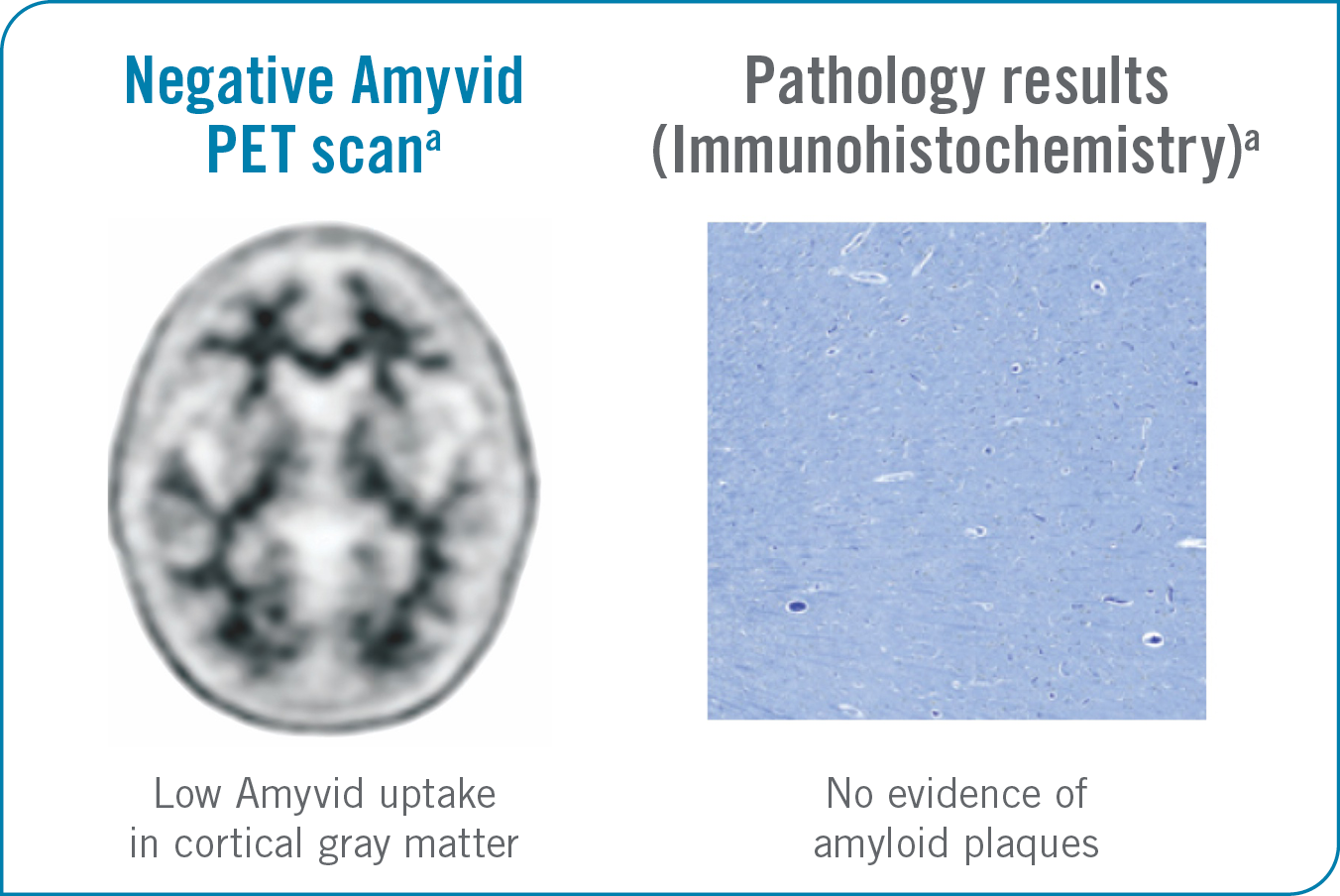
A Negative Amyvid PET Scan2
- Shows more Amyvid uptake in white matter than in adjacent cortical gray matter, creating clear gray-white contrast1,2
- Indicates sparse-to-no amyloid-beta neuritic plaques1,2
- Is inconsistent with a neuropathological diagnosis of AD1
- Reduces the likelihood that cognitive impairment is due to AD1
- Supports the choice to assess other causes of cognitive impairment and potentially avoid unnecessary treatment3,4
- Does not preclude the accumulation of amyloid beta in the brain in the future1
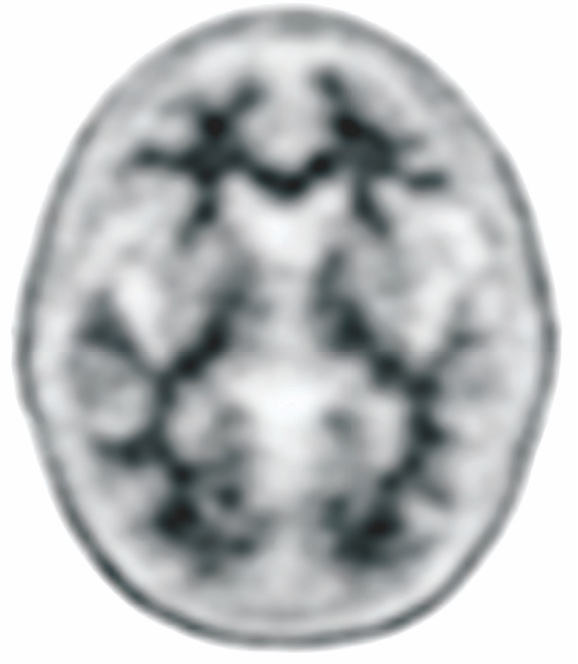
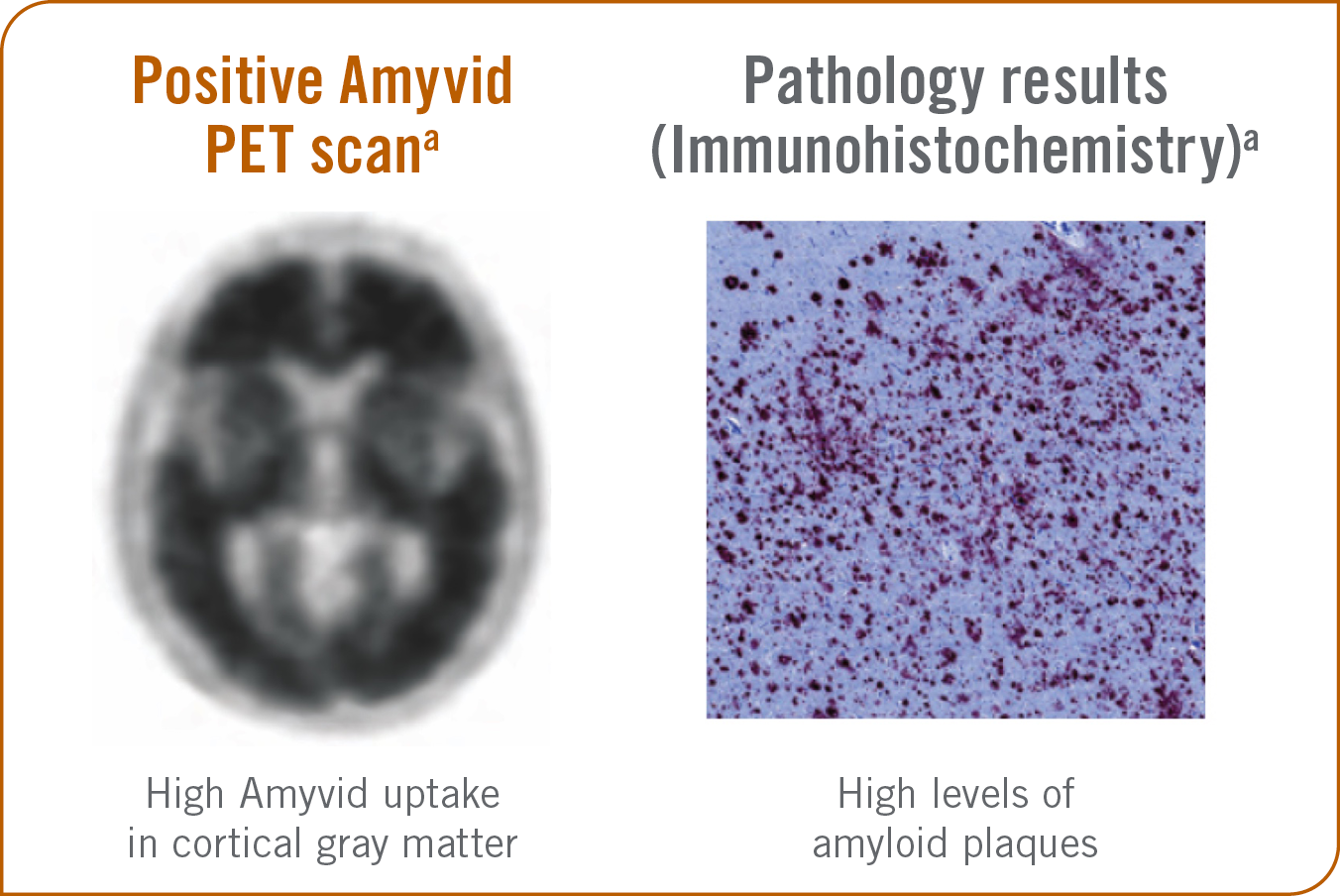
A Positive Amyvid PET Scan5
- Shows high Amyvid uptake in cortical areas with reduction or loss of the normally distinct gray-white contrast. These scans will have 1 or more areas with increased cortical gray matter signal which results in reduced (or absent) gray-white contrast1,5
-
Establishes the presence of moderate-to-frequent amyloid-beta neuritic plaques1,5
- It has been shown that this amount of amyloid beta neuritic plaques was present in patients with AD, but may also be present in patients with other types of neurologic conditions, as well as older people with normal cognition1
- In conjunction with clinical assessment, positive scan results can help you evaluate AD and other causes of decline and in selecting patients who are indicated for amyloid beta–directed therapy1
©2011. Avid Radiopharmaceuticals, Inc. All rights reserved.
The objective of Amyvid image interpretation is to provide an estimate of the brain amyloid-beta neuritic plaque density. Image interpretation is performed independently of a patient’s clinical features and relies upon the recognition of unique image features. Quantitative software may be used in conjunction with the visual read to assess amyloid beta plaque levels.1
Specifically, a positive scan will have either1:
- Two or more brain areas (each larger than a single cortical gyrus) in which there is reduced or absent gray-white contrast. This is the most common appearance of a positive scan.
or
- One or more areas in which cortical gray matter signal is intense and clearly exceeds the signal in adjacent white matter.
Amyvid clinical studies1:
- Amyvid was evaluated in 2 clinical studies that examined subjects with a range of cognitive function, including some terminally ill subjects who had agreed to participate in a postmortem brain donation program as well as healthy subjects
- Both were single-arm studies in which subjects underwent an Amyvid injection and scan. The images were interpreted using a clinically applicable binary image interpretation method (negative or positive) by 5 independent readers who were blinded to all clinical information
- Image interpretations used co-registration with CT scans when PET scans were performed on dual PET-CT scanners
- Before image interpretation, all readers underwent special training on image interpretation: in-person training or electronic media training
SELECT IMPORTANT SAFETY INFORMATION
Risk for Image Misinterpretation and Other Errors
- Errors may occur in the estimation of brain amyloid beta neuritic plaque density during Amyvid image interpretation.
- The use of clinical information in the interpretation of Amyvid images has not been evaluated and may lead to an inaccurate assessment. Extensive brain atrophy as well as motion artifacts that distort the image may limit the ability to distinguish gray and white matter on an Amyvid scan.
Perform image interpretation independently of the patient’s clinical information. For cases where there is uncertainty as to the location of cortical signal, use co-registered anatomical imaging to improve localization of signal.
THE ACCURACY OF AMYVID1
Amyvid demonstrated accuracy for estimating amyloid beta–neuritic plaque density1
Objective evidence of amyloid pathology based on autopsies performed within 2 years of Amyvid scan (n=59)1
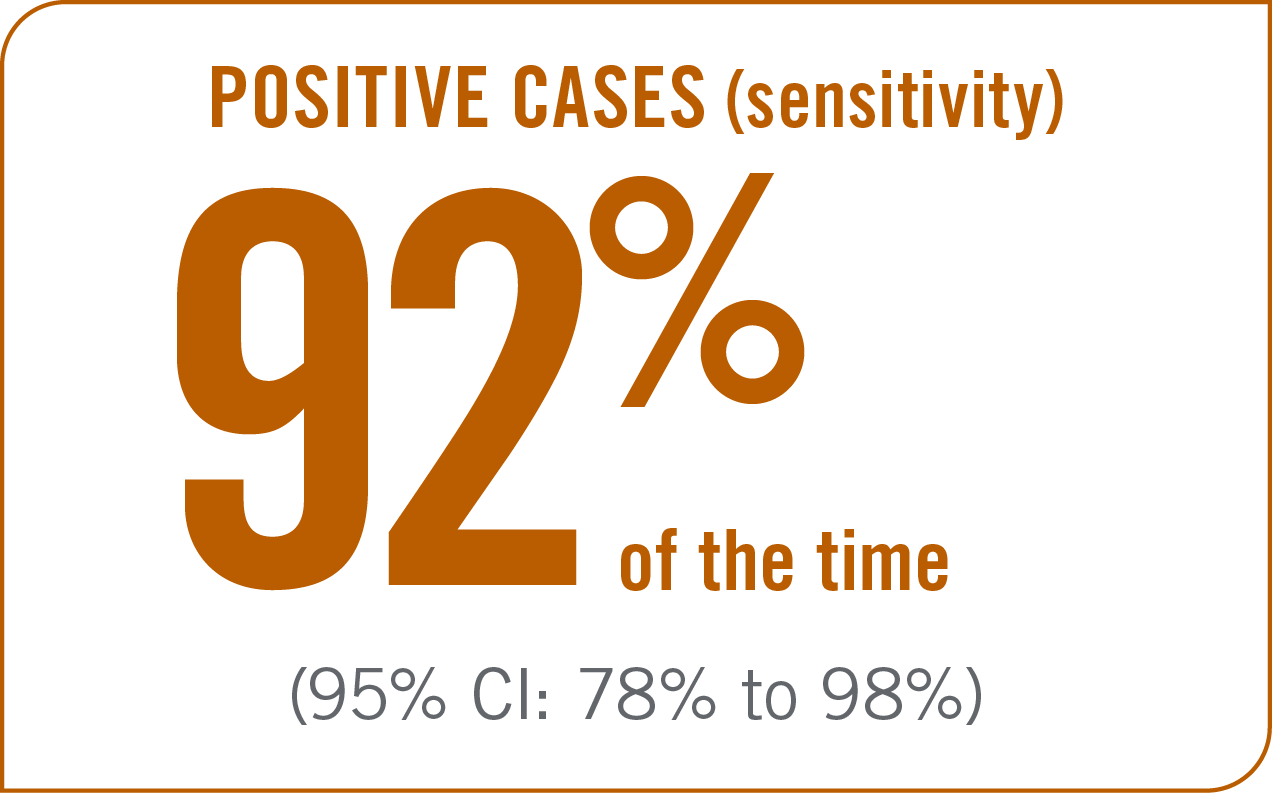
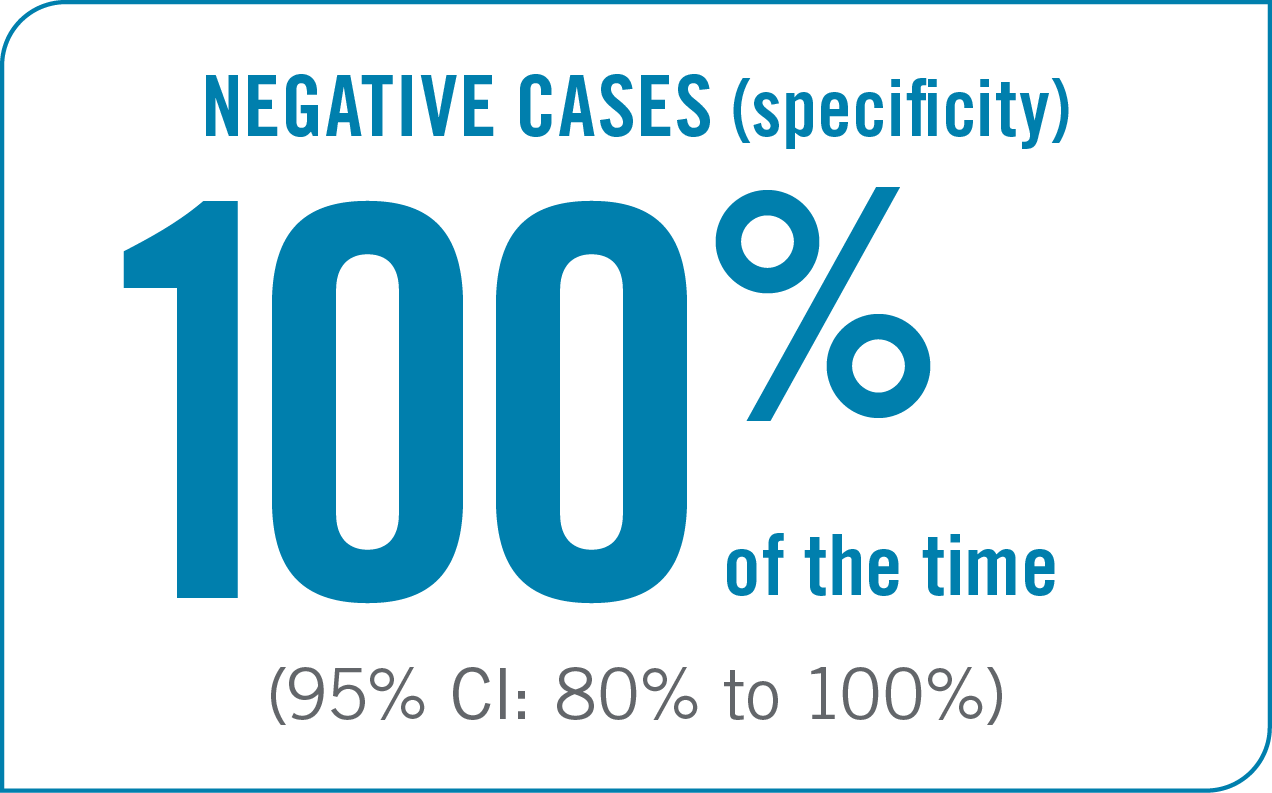
In a Clinical Trial, Amyvid identified:1
Study 1:
Assessed the sensitivity and specificity of a binary visual read methodology in patients who underwent autopsy compared to a postmortem truth standard.1
Design:
- 5 readers (trained in person)
- Binary visual read methodology
Population:
- 59 terminally ill patients who received premortem Amyvid scans and then underwent autopsy
- Of these 59 patients, 29 patients had an AD clinical diagnosis, 13 had another type of dementing disorder, 12 had no history of cognitive impairment, and 5 had MCI
Results:
- In patients who had an autopsy within 2 years of PET imaging (n=59), sensitivity* was 92% (95% CI: 78% to 98%) and specificity* was 100% (95% CI: 80% to 100%)1
*Sensitivity and specificity were calculated using the majority interpretation of the readers for the presence or absence of moderate-to-frequent amyloid plaques1
SELECT IMPORTANT SAFETY INFORMATION
Radiation Risk
- Amyvid contributes to a patient’s overall long-term cumulative radiation exposure. Long-term cumulative radiation exposure is associated with an increased risk of cancer. Ensure safe handling to protect patients and health care workers from unintentional radiation exposure. Advise patients to hydrate before and after administration and to void frequently after administration
Amyvid provided reliable evidence for amyloid pathology by estimating amyloid beta neuritic plaque density1
Statistically significant correlation between Amyvid PET scan images and amyloid beta neuritic plaque deposition seen at autopsy (Spearman's rho=0.78; 95% CI: 0.58 to 0.89; P<0.0001) (n=29).6
Negative Amyvid PET Scan Results1,2,7
©2011. Avid Radiopharmaceuticals, Inc. All rights reserved.
- Indicates sparse-to-no amyloid plaques1
- Inconsistent with a neuropathological diagnosis of AD1
- Unlikely that cognitive impairment is due to AD1
aThese are examples of a negative amyloid PET scan and pathology slide with no evidence of amyloid plaques.2,7
Positive Amyvid PET Scan Results1,5,7
©2011. Avid Radiopharmaceuticals, Inc. All rights reserved.
- Indicates moderate to frequent amyloid plaques1
- Is consistent with a neuropathological diagnosis of AD1
- This amount of amyloid plaque is seen in patients with AD, but may also be present in patients with other conditions as well as cognitively normal older people1
aThese are examples of a positive amyloid PET scan and pathology slide with high levels of amyloid plaques.5,7
A clinical study assessed the correlation between amyloid plaques seen at autopsy and estimates for beta-amyloid neuritic plaque density using Amyvid PET imaging.6
Design:
- 3 readers; semiquantitative reading methodology (not intended for clinical use).6
Population:
- 35 terminally ill patients who received premortem Amyvid scans and then underwent autopsy (29 of which comprised the primary analysis set).6
SELECT IMPORTANT SAFETY INFORMATION
Risk for Image Misinterpretation and Other Errors
- Errors may occur in the estimation of brain amyloid beta neuritic plaque density during Amyvid image interpretation.
- The use of clinical information in the interpretation of Amyvid images has not been evaluated and may lead to an inaccurate assessment. Extensive brain atrophy as well as motion artifacts that distort the image may limit the ability to distinguish gray and white matter on an Amyvid scan.
Perform image interpretation independently of the patient’s clinical information. For cases where there is uncertainty as to the location of cortical signal, use co-registered anatomical imaging to improve localization of signal.
The reproducibility of Amyvid1,8
Amyvid has been shown to have high inter-reader reproducibility for estimating amyloid-beta neuritic plaque density1,8
High inter-reader reproducibility
- 92% of interpretations agreed with the majority (95% CI: 89.8% to 94.1%) (n=59)8
- Overall Fleiss' kappa statistic† of 0.83 (95% CI: 0.78 to 0.88) (n=151); the lower bound of the 95% CI exceeded the prespecified success criterion of 0.581
Study 1: assessed the sensitivity and specificity of a binary visual read methodology in patients who underwent autopsy compared to a postmortem truth standard.1
Design:
- 5 readers (trained in person)
- Binary visual read methodology
Population:
- 59 terminally ill patients‡ who received premortem Amyvid scans and then underwent autopsy
Study 2: assessed the inter- and intra-reader image interpretation reproducibility in subjects with and without autopsy.1
Design:
- 5 readers (electronic media training)
- Binary visual read methodology
Population:
- 92 subjects§ who did not undergo autopsy in addition to 59 patients (same population from Study 1) with autopsy data
- 33 images were used to assess intra-reader reproducibility
†Fleiss’ kappa: the degree of agreement among multiple readers over that which would be expected by chance.
‡Twenty-nine (29) patients had an AD clinical diagnosis, 13 had another type of dementing disorder, 5 had MCI, and 12 had no history of cognitive impairment.1
§Twenty (20) with AD, 52 patients with MCI, 20 healthy volunteers.1
SELECT IMPORTANT SAFETY INFORMATION
Risk for Image Misinterpretation and Other Errors
- Errors may occur in the estimation of brain amyloid beta neuritic plaque density during Amyvid image interpretation.
- The use of clinical information in the interpretation of Amyvid images has not been evaluated and may lead to an inaccurate assessment. Extensive brain atrophy as well as motion artifacts that distort the image may limit the ability to distinguish gray and white matter on an Amyvid scan.
Perform image interpretation independently of the patient's clinical information. For cases where there is uncertainty as to the location of cortical signal, use co-registered anatomical imaging to improve localization of signal
Learn more about the Amyvid procedure time
PROCEDURE TIMECI=confidence interval; CT=computed tomography; MCI=mild cognitive impairment; PET=positron emission tomography.
References:
- Amyvid (florbetapir F 18 injection). Prescribing Information. Lilly USA, LLC.
- Data on File. Lilly USA, LLC. DOF-AM-US-0008.
- Weidman DA, Zamrini E, Sabbagh MN, et al. Added value and limitations of amyloid-PET imaging: review and analysis of selected cases of mild cognitive impairment and dementia. Neurocase. 2017;23(1):41-51. doi:10.1080/13554794.2017.1290806
- Shea YF, Barker W, Greig-Gusto MT, et al. Utility of amyloid PET scans in the evaluation of patients presenting with diverse cognitive complaints. J Alzheimers Dis. 2018;66(4):1599-1608. doi:10.3233/JAD-180683
- Data on File. Lilly USA, LLC. DOF-AM-US-0007.
- Clark CM, Schneider JA, Bedell BJ, et al; for AV45-A07 Study Group. Use of florbetapir-PET for imaging β-amyloid pathology. JAMA. 2011;305(3):275-283.
- Data on File. Lilly USA, LLC. DOF-AM-US-0006.
- Data on File. Lilly USA, LLC. DOF-AM-US-0005.